

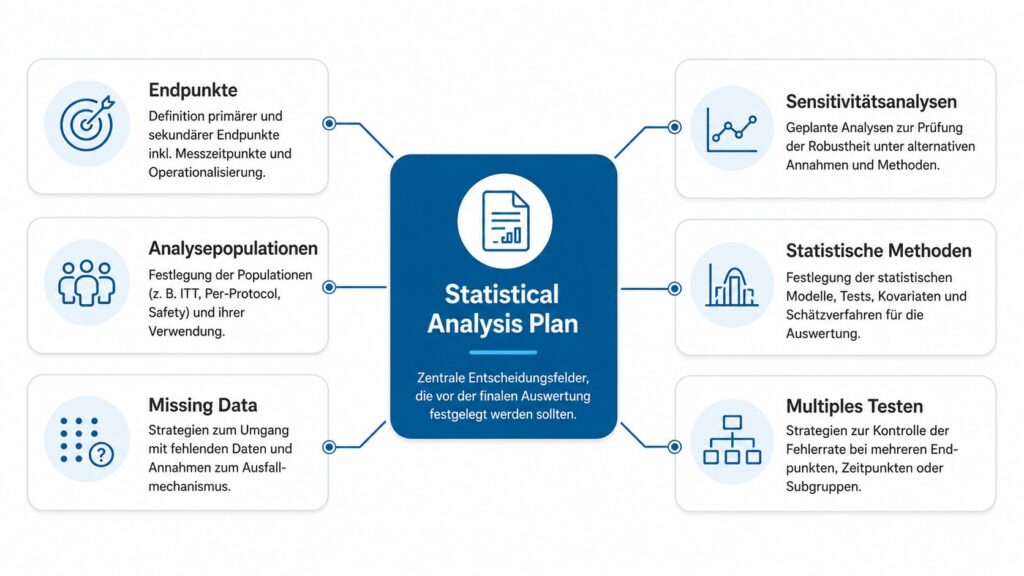
A Statistical Analysis Plan (SAP) describes in advance how clinical study data will be statistically analyzed. Among other things, it defines endpoints, analysis populations, statistical methods, missing data strategies and sensitivity analyses before the final results are known.
In clinical trials, the SAP is therefore more than just a technical document. It protects the evaluation from retrospective decisions, reduces scope for interpretation and creates a reliable basis for the study report, publication and regulatory assessment.
Regulatory guidelines such as ICH E9 therefore expect key analysis decisions to be defined before the database is closed and before the final results are known. These include endpoint definitions, analysis populations, missing data strategies and the handling of multiple statistical tests.
What is a statistical analysis plan?
A statistical analysis plan is a detailed analysis plan for clinical study data. It supplements the study protocol and describes how statistical analyses are to be carried out in concrete terms. While the study protocol primarily defines medical and organizational aspects of a study, the SAP describes the statistical implementation. This includes, among other things
- Analysis populations,
- Endpoint definitions,
- statistical models,
- Missing data strategies,
- Sensitivity analyses,
- as well as planned tables and presentations of results.
The SAP thus serves as a binding basis for the subsequent statistical evaluation of a clinical study.
Why is SAP so important in clinical trials?
Clinical studies generate a large number of potential evaluation options. Even small changes in analysis populations, endpoint definitions or statistical models can visibly influence results.
SAP reduces this risk by defining central decisions before the actual analysis. This makes it clear which analyses were actually planned and which evaluations are exploratory in nature. This is particularly relevant for:
- multiple endpoints,
- several analysis points in time,
- Subgroup analyses,
- Missing Data,
- Protocol Deviations,
- or complex study designs.
Without clear preliminary definitions, scope for interpretation quickly arises. Results can then be consciously or unconsciously presented selectively. It is precisely this risk that the SAP aims to limit. This traceability plays a central role in regulatory studies in particular. Authorities expect statistical decisions to be reproducibly documented and professionally justified.
What content should be included in a statistical analysis plan?
The specific structure of an SAP can vary depending on the study. However, some components are relevant in almost all clinical trials. These include information on the study objective, study design, endpoints and analysis populations. A distinction is often made between intention-to-treat, per-protocol, safety population or other study-specific populations.
The statistical methods are another key component. The SAP describes which tests, models or estimation methods are used for primary and secondary endpoints. It should also specify which covariates are taken into account and how confidence intervals, p-values or effect measures are reported.
In many clinical studies, specific modeling strategies are also defined, for example ANCOVA models, mixed models for repeated measures or Cox regressions for time-to-event endpoints. Rules for subgroup analyses, visit windows, protocol deviations or intercurrent events should also be described in a comprehensible manner.
With ICH E9(R1), the precise definition of so-called estimands has also gained in importance. This involves the question of which treatment effect should actually be estimated under which conditions, for example in the case of treatment discontinuations, rescue medication or other intercurrent events. SAP often forms the operational basis for implementing these definitions statistically.
Equally important are rules for missing data. Missing data can significantly influence study results. The SAP should therefore not only mention that missing values can occur, but also describe specifically how they are handled and which sensitivity analyses are planned.
Tables, listings and illustrations can also be planned in SAP. This sounds technical, but it is practically relevant: A clear results structure prevents evaluations from being unsystematically expanded or selectively highlighted later on.
When the Statistical Analysis Plan should be created
An SAP should be finalized before the final data analysis. In many clinical trials, it makes sense to finalize the SAP before database closure or at least before unblinding. The exact timing depends on the study design. However, the principle is crucial: the key analysis decisions must be made before knowledge of the results could influence these decisions.
SAPs that are created too late lose some of their methodological value. If analysis populations, exclusion rules or sensitivity analyses are only formulated after the data has been viewed, a credibility problem arises that is difficult to resolve. This can be critically questioned later in regulatory procedures. Changes to primary analyses after the data has been reviewed are considered particularly sensitive because they can call the objectivity of the evaluation into question.
In practice, the SAP should therefore not be regarded as the last formality. It belongs in the study planning and should be closely coordinated with the protocol, data management, monitoring, statistical programming and data integrity.

Typical SAP errors in practice
A common mistake is to formulate the SAP too generally. Statements such as “the data are analyzed descriptively and inferentially” are not sufficient for a clinical study. They leave open which analysis is actually relevant.
Unclear endpoint definitions are also problematic. If it is not clearly defined which measurement time point, which analysis window or which operationalization applies, there is room for interpretation later on.
Analysis populations are also critical. Particularly in the case of deviations from the protocol, dropouts or incompletely documented visits, it must be clear which patients are included in which analysis. Without these rules, results may vary depending on the population.
Missing data is also often underestimated. Missing values are not only a data problem, but also a methodological risk for the interpretability of the results. Different assumptions about the failure mechanism can lead to significantly different results. The SAP should therefore determine as early as possible whether, for example, multiple imputation, mixed models or other methods are planned and how sensitivity analyses should check the robustness of the results.
Additional analyses that are not clearly categorized are also problematic. Subgroup analyses, exploratory endpoints or alternative model variants can be useful. However, they should be clearly distinguished from the primary analyses and not subsequently change the character of the main analysis.
Connection with endpoints, missing data and sensitivity analyses
Many methodological problems in clinical studies only become apparent when data is incomplete or results are inconclusive. This is precisely why it is not enough to describe statistical methods only roughly.
The SAP should provide comprehensible documentation:
- which endpoints are primarily relevant,
- which analyses are interpreted in a confirmatory or exploratory manner,
- which assumptions are made about missing data,
- and how sensitivity analyses test the robustness of the results.
Endpoints and analysis populations
Endpoints and analysis populations are among the most important methodological specifications of an SAP. Even small changes can influence the interpretation of clinical results.
The clear distinction between primary and secondary endpoints is particularly relevant here. While primary endpoints are intended to answer the central clinical question, secondary endpoints are often used for supplementary classification or exploration.
Analysis populations must also be precisely defined. Differences between intention-to-treat, per-protocol or safety analyses can lead to different results. The SAP should therefore transparently define which population is relevant for which question.
Missing data and sensitivity analyses
Sensitivity analyses are particularly important for assessing the robustness of clinical results. They show whether central results remain stable when alternative assumptions or analysis approaches are used.
This applies, for example:
- alternative imputation methods,
- different analysis populations,
- alternative covariate structures,
- or different definitions of clinical endpoints.
Without these preliminary definitions, the impression of data-driven decisions is quickly created. SAP creates methodical traceability here and reduces the risk of selective interpretation.
Multiple testing and error rates
Clinical studies often examine several endpoints, time points or subgroups simultaneously. Without suitable strategies, this increases the risk of random statistical significance.
The SAP should therefore clearly describe how multiple testing is controlled, for example by hierarchical testing strategies or other methods to control alpha error accumulation. Especially for secondary endpoints and exploratory analyses, this classification is crucial for the subsequent interpretation of the results.
Conclusion
A statistical analysis plan is a key instrument for making clinical study evaluations plannable, comprehensible and methodologically robust. Prior to the analysis, it determines how endpoints, analysis populations, missing data, sensitivity analyses and presentation of results are to be handled.
Its value lies above all in reducing the scope for interpretation later on. Particularly in complex clinical trials, a well-developed SAP prevents statistical decisions from being made only after the results have been seen.
In regulatory studies in particular, the quality of the SAP often determines whether results are later accepted as reliable and comprehensible. Many methodological problems in clinical trials do not only arise during the evaluation, but also as a result of unclear or subsequently changed analysis decisions.
A precise SAP reduces this risk and creates the basis for reproducible and technically convincing study results.
Further reading:
Fradera, M., & Serra-Aracil, X. (2025). Statistical Analysis Plan (SAP): What is it and how to develop it?. Cirugia espanola, 103(1), 45-48. https://doi.org/10.1016/j.cireng.2024.07.007
International Council for Harmonization (ICH). (1998). ICH E9 statistical principles for clinical trials. European Medicines Agency. https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-9-statistical-principles-clinical-trials-step-5_en.pdf
Yale School of Public Health. (n.d.). Statistical analysis plans. Yale Center for Analytical Sciences. https://ysph.yale.edu/ycas/dcc/saplans/